
Pelvic Organ Prolapse
What Can Be Done to Prevent It?
The word “prolapse” comes from a Latin word meaning “to fall out of place,” which is an apt description of what happens with pelvic organ prolapse, or POP. POP occurs when an organ in the pelvic region (typically the bladder, uterus, or part of the vagina) “falls” and shifts position, sometimes protruding outside of the vagina. Urinary incontinence is the most common symptom of POP.
As of 2009, approximately 3.3 million women in the US alone were estimated to be affected by POP. Based on census data and an aging population, the incidence of women with POP is expected to increase dramatically. By the year 2050, the number of women undergoing surgery for POP is projected to increase by nearly 50%. This data forewarns us that approximately 1 out of every 5 women in the US will undergo some sort of surgery for pelvic organ prolapse in her lifetime. That’s a lot of POP—and a lot of surgery!
So why have so few women heard of pelvic organ prolapse? That’s one of the questions Sherrie Palm asked when she was faced with it herself. This newsletter started out as a review of her book, Pelvic Organ Prolapse: The Silent Epidemic, in which she shares her personal history (including a hysterectomy and subsequent POP), her quest for information, her decision to have surgery to correct POP, and the aftermath of that surgery. Her book will undoubtedly prove to be a valuable resource to many women experiencing POP or considering a hysterectomy.
In reading through Sherrie’s book, as well as others on the topic, we found ourselves also asking: Why?
- Why do so many women experience prolapse?
- Who do so few women (even medical professionals) talk about prolapse?
- Why do so many women have surgery?
- Why do so many women regret having that surgery, even though it may have “fixed” their symptoms?
We think the answers to these questions are important to explore, with the hope that it might mean that fewer women will experience pelvic organ prolapse and that fewer women will have to face a difficult decision regarding pelvic surgery.
First, we will review definitions and provide a little background on pelvic organ prolapse (POP).
Types of Pelvic Organ Prolapse
There are different types of prolapse (see figures) and all can occur in varying degrees. Some women experience no symptoms, while the symptoms for others can be debilitating and life-altering.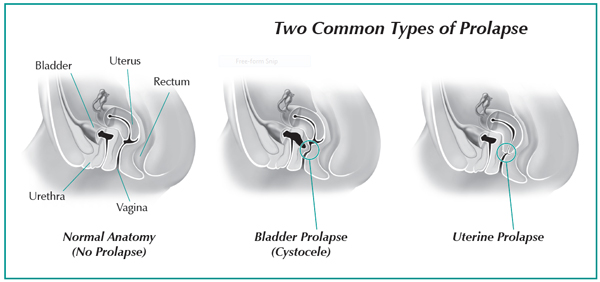
Bladder prolapse (cystocele) is the most common form and is frequently accompanied by urinary incontinence. If the muscles and connective tissue that hold the bladder in place become weak, stretched, or injured, the bladder can fall away from its natural spot and press against the vaginal wall, causing discomfort and potentially forming a bulge in the vagina. The urethra can also collapse (urethrocele) if not properly supported by the muscle tissue around it.
Uterine prolapse can occur if the muscles and ligaments of the pelvic floor and surrounding tissue are weak. Without enough support, the uterus may fall from its normal position into the cervix, creating a bulge in the vagina.
Vaginal prolapse (also called vaginal vault prolapse) is quite common after a hysterectomy (surgery to remove the uterus), but not everyone who has a hysterectomy experiences POP. Without the uterine attachments to hold it up, the top of the vagina can drop into the vaginal canal.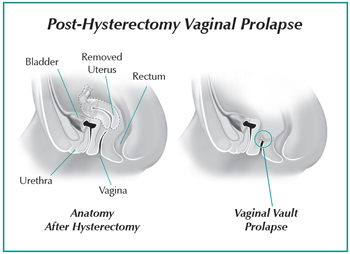
Other forms of prolapse (not shown) involve the small bowel (enterocele) and rectum (rectocele). If the tissues and muscles surrounding these areas become weak or damaged, they also can fall against the wall of the vagina, causing pressure or a bulge.
Primary Causes
The precise cause of pelvic organ prolapse may be hard to determine, as there are often multiple factors at work, including genetics, vaginal childbirth, hysterectomy or other pelvic surgery, obesity, heavy lifting, chronic cough, chronic constipation, and age-related hormone loss or other hormone imbalances.
Childbirth
The majority of women with POP most likely have given birth to one or more children. The stress on connective tissue as the baby grows, the pressure of the uterus and increasing weight on the pelvic floor, the abdominal strain during labor, and general trauma to the overall pelvic region during vaginal delivery all enhance the risk of POP.
Surgical repair after childbirth is common, but not always effective. The repair itself can lead to other discomfort or health problems, and subsequent surgery, especially if the mesh fails or the patient has an allergic reaction to the mesh.
Hysterectomy
The other primary cause of POP is hysterectomy. There is much debate about the need for hysterectomies and some speculation that it is over-prescribed as the solution to many female health conditions.
Many women experience heavy menstrual bleeding or intense cramps for years, or are diagnosed with fibroids or endometriosis, and are basically told to “wait and see” until it becomes too much to bear. When they can’t take it anymore, it becomes an emergency situation with an extreme solution: hysterectomy. Unfortunately, the repercussions of hysterectomy are often trivialized, and the short-term success stories are colored by the immediate effects of being pain-free; but the long-term consequences eventually take their toll.
It should be no surprise that, if you remove organs from the pelvic region, it leaves a void that the body will try to compensate for by shifting the remaining organs, muscles, and tissues. With the number of hysterectomies performed in the US alone, why aren’t more women warned that pelvic organ prolapse is a possible result?
Sources for both pre- and post-surgery support include the Hysterectomy Educational Resources and Services (HERS) Foundation, the Whole Woman Blog, and the online support group, HysterSisters. One quote from Whole Woman sums it up: “Alternative treatments are useful experiments to see what can help. Surgery is not an experiment. It is a decision you will have to live with the rest of your life.”
Kegel Exercises: Do they work for prolapse?
Most women with POP find that Kegel exercises do not help, and may even make their situation worse. As with any exercise, the body needs the proper hormones, such as DHEA and testosterone, as well as the proper nutrients to rebuild the muscles. If hormone or nutrient deficiency is part of the underlying cause for the prolapse in the first place, Kegel’s will not save the day.
Yoga, pilates, swimming, and other exercises that focus on the core have proven to be helpful for many women with POP. Another non-surgical alternative is a pessary, which is a device similar to a diaphragm, which when inserted into the vagina helps support the uterus or vaginal wall to prevent or minimize prolapse.
For many women, the risk of POP can be mitigated by properly maintaining the pelvic floor, which is the foundation of the internal organs. Adequate exercise, proper nutrition, and hormone balance are all part of keeping the core muscles and tissues healthy and stable, so they can support the rest of the body.
NOTE: We are not advising against or for hysterectomy. Each woman should confer with her healthcare professionals and make that decision based on her own personal situation, and there are certainly situations where it IS the best or only solution. Even Sherrie Palm, knowing what she knows now, feels she would do it all over again. However, now that she is informed about POP and is actively sharing that information with others, Sherrie hopes more women will have a better idea of what to expect—and how to prepare for it—before being forced to make that decision for themselves.
Associated Conditions
Pelvic organ prolapse often occurs in conjunction with a number of different health conditions—most of which relate to a hormone imbalance—including fibroids, endometriosis, hypothyroidism, multiple sclerosis and Vitamin D deficiency, among others. Taking a proactive approach to regaining hormone balance, maintaining proper posture, and properly improving the strength of the pelvic muscles may help reduce the likelihood of POP.
Fibroids / PCOS / Endometriosis / Adenomyosis
Sherrie’s decision to have a hysterectomy was driven by a diagnosis of fibroids and a cystic ovary. Unfortunately, this is an all too common path for many women. What they may not realize is that these types of conditions are typical symptoms of hormone imbalance, which could have been diagnosed and corrected long before hysterectomy became the only option.
Hypothyroidism
Many women who experience POP may also have exhibited symptoms of hypothyroidism, even from an early age. The Broda Barnes Research Foundation recognizes constipation, cystic breasts and ovaries, and infertility as signs of hypothyroidism, and these same symptoms are also known to be precursors to prolapse. Additional examples of symptoms related to both conditions include extreme ligament laxity or hypermobility (such as being able to touch your thumb to your forearm), muscle weakness, flat feet (essentially weak ligaments in the feet) and scoliosis (ligaments too weak to maintain the proper posture of the spinal column).
Multiple Sclerosis
Like Sherrie, who was diagnosed with multiple sclerosis (MS) at the age of 30, many women with MS also experience POP, even without having had a hysterectomy. Is it any wonder that, after a hysterectomy, a body predisposed with this disease can’t hold the rest of the organs in place?
According to Dr. Ray Peat, the destructive process that is MS is characterized by high estrogen levels, low thyroid levels, and poor absorption of amino acids from protein. This combination hinders the formation of structural tissue. Also highly characteristic in people with MS are high levels of cortisol, which leads to the breakdown of muscles, ligaments, cartilage, and bone.
In addition, women with MS are also often deficient in the hormones progesterone and pregnenolone, which are anti-inflammatory and necessary for the myelin sheath protecting nervous system tissue. Deficiencies of these same hormones are also associated with the development of fibroids and ovarian cysts, as well as issues with infertility.
Vitamin D Deficiency
Research indicates that adequate Vitamin D is essential for maintaining pelvic health. Studies demonstrate that the risk of pelvic disorders in women of all ages is significantly reduced when Vitamin D levels are high (30 ng/mL or higher in one study), and more prevalent when Vitamin D levels are low. Vitamin D deficiency has also been linked to Inflammatory Bowel Disease (IBS), a symptom Sherrie also exhibited for years before her hysterectomy and POP.
Conclusion
It is ironic that most of us recognize the importance of regular maintenance on our homes and cars, but take a “wait and see” approach when we get warning signals about our health. Many women experience heavy menstrual bleeding or intense cramps for years, or are diagnosed with fibroids or endometriosis, and are basically told to wait until it becomes too much to bear. When they can’t take it anymore, it becomes an emergency situation with an extreme solution: a hysterectomy.
If you decide to have a hysterectomy, taking care to proactively maintain the strength of the pelvic infrastructure before and after surgery will help with the recovery, as well as reduce the risk of pelvic organ prolapse.
The information on this website is for informational purposes only and is not intended to be a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified healthcare provider with any questions you may have regarding any condition or medication. Do not disregard professional medical advice or delay in seeking it because of something you have read on this site.
