
High Blood Pressure
A Symptom, Not a Disease
As of 2013, approximately 30% of Americans over the age of 20, and over 50% of those age 55 and older, have elevated blood pressure or hypertension. While not a disease in and of itself, high blood pressure is strongly associated with conditions affecting the heart and vascular system health. Because hypertension usually produces no telltale symptoms, many people do not realize they have it. When people are diagnosed, in all but a small percentage of cases, the underlying cause is unknown.
It seems incredible that a condition with no known cause and no overt symptoms would receive aggressive medical attention. Yet hypertension is considered so predictive of heart attack and stroke that when diet and exercise changes do not work, one or more medications are nearly always prescribed, despite the potential for serious side effects.
Instead of a single-minded focus on lowering blood pressure, Cass Ingram, DO, says medicine must take a broader approach to improving the entire vascular system’s health. “There are no drugs which heal or cleanse the heart and arteries,” he writes. “Only a natural approach can heal.”
How Blood Circulates: A Pressure Balance
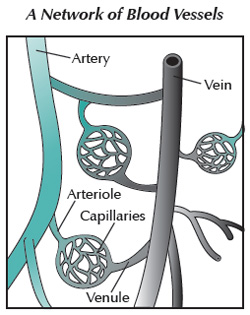 The vascular system (also known as the circulatory system) is made up of the heart and blood vessels, which can be thought of as a network of flexible tubes, arranged in a tree-like structure from the largest vessels (veins and arteries) narrowing to smaller venules and arterioles. These are connected by capillaries, thread-like vessels where blood flows slowly enough to enable the exchange of gas and nutrients between blood and the surrounding tissue.
The vascular system (also known as the circulatory system) is made up of the heart and blood vessels, which can be thought of as a network of flexible tubes, arranged in a tree-like structure from the largest vessels (veins and arteries) narrowing to smaller venules and arterioles. These are connected by capillaries, thread-like vessels where blood flows slowly enough to enable the exchange of gas and nutrients between blood and the surrounding tissue.
The heart serves as a pump to move blood through the vessels. Veins bring carbon dioxide-filled blood from our tissues back to the heart. The heart pumps blood to the lungs to pick up oxygen and release carbon dioxide. Blood returns to the rest of the body via the other large set of “tubes”—the arteries.
Because it is a closed loop system, pressure develops, which is necessary to keep blood flowing continuously against the force of gravity. Achieving the proper balance of pressure is very important. While uncommon, there are some conditions, such as adrenal gland dysfunction, that can cause blood pressure to drop too low, causing dizziness and fainting.
What is High Blood Pressure?
Blood pressure is the force that blood exerts on the walls of your arteries. Readings of this pressure are given as a fraction and measured in millimeters of mercury, such as 120/80 mmHg. The top number refers to the force when your heart beats; the bottom number is the force when your heart rests. For most adults, readings of 120/80 or less are considered healthy. A reading of 140/90 or higher is usually considered hypertensive. Revised U.S. guidelines published in 2003 added a new category: prehypertension, defined as all the readings in between, because even small increases in blood pressure appear to correlate to increased disease risk.
In people with arteriosclerosis (the general term for hardened, narrowed arteries), blood pressure rises in order to compensate. The heart must work harder to move blood through the tightened arteries, which weakens it over time. Naturally, the arteries also take a pounding. High blood pressure is a strong signal that help is needed to restore optimal vascular function.
Every cell in the body—from toenail to brain—is nourished with oxygen and nutrients from the blood. When blood flows properly through the circulatory system, body processes are properly fueled and toxins are removed as blood is filtered through the liver and kidneys.
But as people age, damage to blood vessels often occurs, making those vessels less efficient in transporting blood. Over time, hypertension and poor blood circulation can lead to a wide variety of health problems, including:
- Plaque buildup in blood vessel walls
- Kidney failure
- Leg pain
- Memory problems
- Heart attacks
- Stroke
Researchers are just beginning to determine the chain of events that leads to vascular disease. While many links in the chain have been clearly identified, other links are just being discovered. Yet the real difficulty lies in separating these discoveries into causes and effects. In many cases, researchers simply know that certain things go together—that many people with high cholesterol levels, for example, also have poor circulation, making each a “risk factor” for the other. But that doesn’t tell us whether high cholesterol causes poor circulation or is in fact caused by it, or if it’s just a symptom of another underlying cause.
Hunting Down the Causes
A medical mystery like hypertension attracts many researchers eager to solve it. Dozens of theories have been proposed to explain the details of how hypertension develops. Many think multiple causes are at work because the treatments shown to help lower high blood pressure in individuals include more than 100 different medications, as well as supplements and lifestyle changes. Yet for many, a cure proves elusive, particularly when the standard medications may not be well tolerated.
Some people even find that anti-hypertensive drugs can make the problem worse. Sherry A. Rogers, MD, describes the common scenario where physicians prescribe diuretics (medications that reduce water and salt), thus lowering the total volume of blood flowing through the vessels, which lowers the pressure, the same way turning down your spigot reduces the pressure in a garden hose. Unfortunately, diuretics may also create imbalances such as a depletion of potassium. “For some folks, an improperly diagnosed potassium deficiency is often the underlying cause of the high blood pressure,” she explains in The High Blood Pressure Hoax. “Taking a medication that silently lowers potassium even further leads to higher blood pressure and guarantees the need for even stronger medications in a few years.”
This brings us to our interest in understanding more about the factors that affect blood pressure. The following theories show promise for restoring normal blood pressure and improving vascular function.
The Hormone Connection
The incidence of high blood pressure in women increases dramatically after menopause, suggesting a connection to hormones. As the body’s chemical messengers, hormones orchestrate our metabolic processes by stimulating changes in cells—including those in our blood vessels. Hormones, which originate in various glands, circulate throughout the body in the blood, bathing our tissues. Receptors within our cells are sensitive to particular hormones, causing a reaction.
In our blood vessels, receptor cells are particularly sensitive to several hormones, including estrogens, progesterone, testosterone and cortisol. They are also very sensitive to a steroid hormone that acts as a precursor to all of these, called DHEA (dehydroepiandrosterone).
Cardiovascular problems have been linked to deficiencies in DHEA, thyroid, and other hormones, including Vitamin D. Both heart rate and arterial tone are controlled by the glands, says Dr. Ingram. “It is the disruption of glandular function that is at issue…when this system is dysfunctional, blood pressure disorders develop.”
Estrogens and Progesterone
For decades, estrogens have been thought to protect premenopausal women from heart disease. The theory was simple: estrogens lower “bad” cholesterol and raise “good” cholesterol, reducing atherosclerosis—the buildup of plaque in artery walls that causes them to harden, narrowing and restricting blood flow to the body’s tissues.
Researchers were so excited by this theory that they proposed that menopausal women consider hormone therapy solely to protect heart health. However, when the national Women’s Health Initiative (WHI) ran a large clinical trial to test this theory from 2002–2004, they found that participants taking Prempro, a combination of synthetic progestin and estrogens derived from horse urine (Premarin), actually showed a slight increase in heart attacks, stroke, blood clots and breast cancer. However, there were several limitations to this study, such as the fact that the progestin used in the WHI study was previously linked to coronary artery spasms, while progesterone itself relaxes the arteries.
Research indicates that Premarin alone, or Premarin combined with biologically identical progesterone, may be more effective in increasing HDL (good cholesterol) than Prempro. In fact, results from an ancillary study of WHI participants, published by the New England Journal of Medicine in June 2007, found that women aged 50 to 59 who received estrogen (Premarin) had lower levels of calcified plaque in their coronary arteries, compared to participants who received a placebo. Further research is needed to determine if even better results can be achieved by using only biologically identical hormones.
Although the effects of various estrogen therapies on blood pressure have been controversial, sometimes contradictory, and often confusing, there is reassuring news. In 2006, a University of Wisconsin pharmacy student reviewed several studies and found that postmenopausal women taking biologically identical estrogens and/or progesterone did not have a statistically significant change in blood pressure. Additionally a 2006 editorial in Menopause suggests that “the type of estrogen influences the hypertensive response,” such as estrone and estradiol showing reductions in blood pressure.
Testosterone and Cortisol
For over 40 years, scientists and practitioners have been debating the role of cholesterol in atherosclerosis. Dr. Jens Møller, the former President of the European Organization for the Control of Circulatory Diseases, argues that high cholesterol is a symptom of deterioration in circulation. Dr. Møller details how a deteriorated circulation system and high cholesterol levels can be treated with testosterone to decrease the “stickiness” of the plaque and reduce overall cholesterol levels.
Dr. Møller also reminds us that cholesterol is “the precursor of many hormones, including the vital substance testosterone itself. Decreasing the cholesterol level alone may in fact result in a decrease in the production of testosterone, which plays a vital role in maintaining a normal circulation.” The link between testosterone and the “stress hormone” cortisol provides the mechanism for Dr. Møller’s theory. The problem, he says, is that cholesterol is not a dietary problem, but a sign of a biochemical problem—how the body synthesizes cholesterol.
According to Dr. Møller, excess cortisol is to blame, as it interferes with the normal metabolism of carbohydrates in food, which can lead to insulin resistance and plaque build-up, and eventually cardiovascular disease. The solution, he says, is restoring testosterone, which helps to keep cortisol levels in check.
Thyroid Hormones
Dr. Broda Barnes concurs with the belief that cholesterol is not the cause of heart disease, but a symptom of another problem. In his view, thyroid deficiency is “firmly established as the cause of atherosclerosis.”
In Solved: The Riddle of Heart Attacks, Dr. Barnes reports how atherosclerosis is almost always accompanied by thyroid deficiency, whereas high cholesterol levels, even at an early age, do not necessarily result in a heart attack or cardiovascular disease.
Dr. Barnes claims that thyroid therapy, when given early enough in the course of the disease, prevents cardiovascular disease and increases life expectancy. There is a clear link between thyroid hormones and normal heart function. For example, the majority of thyroid deficient patients exhibit hypertension. There is also a relatively high incidence of heart attacks and strokes among patients with thyroid deficiencies, and an extremely high rate of atherosclerosis among patients who have had their thyroid removed.
DHEA
The adrenal gland hormone DHEA (dehydroepiandrosterone) is a precursor of both testosterone and estrogens. It supports muscle growth and energy metabolism—the rate at which our body absorbs nutrients from our food.
Like testosterone, DHEA is a steroid hormone that acts to balance the effects of the stress hormone, cortisol. It is now well known that chronic stress leads to an outpouring of cortisol, and with that, a gradual depletion of DHEA.
Over time, this hormonal imbalance can lead to hardening of the arteries, thinning bones, increasing waistline girth, and impaired functioning of the immune system. By restoring proper DHEA levels, the normal balance between DHEA and cortisol can be restored.
Chronic Inflammation
DHEA may also help to reduce inflammation. Proper levels of DHEA promote a healthy immune system by helping to achieve the proper balance among the various types of cytokines.
Cytokines are proteins that act as chemical messengers in the body (much like hormones, except that they act locally). They are especially important for regulating inflammatory and immune responses.
As early as the late nineteenth century, a German physiologist proposed that heart disease was caused by inflammation of the heart and arteries. Rudolph Virchow, called the “father of pathology,” originated this theory after noticing that the hearts of deceased heart attack victims looked like bruised and infected flesh, relates Nancy Appleton in Stopping Inflammation: Relieving the Cause of Degenerative Diseases.
Medicine has come back around to Virchow’s view, as there is now widespread acceptance of the role that inflammation plays in the development of atherosclerosis. Research in the 1980s led to the development of this now popular model: inflammatory immune-system cells burrow into an arterial wall, where they are fed by fat deposits. “These cells form a plaque that is weakened by inflammation,” Appleton writes. “Then the fibrous cap ruptures, spilling everything into the bloodstream, including cytokines that encourage blood clotting … thus changing a stable cholesterol plaque into an unstable lesion.”
Appleton also describes newer research linking high blood pressure to high cytokine production (indicating an inflammatory response) and also to allergens. By removing allergens, some people have been able to end their hypertension, possibly by eliminating the trigger to their body’s inflammatory response.
What You Can Do to Enhance Your Vascular Health
Monitor Blood Pressure
Because blood pressure varies depending upon the time of day, as well as your physical activity and stress levels, a single reading may not accurately represent your average blood pressure level. For this reason, Dr. Susan Lark, a researcher in clinical nutrition, recommends using a digital blood pressure machine to check your blood pressure at home, in addition to routine monitoring during medical appointments. When seeing your healthcare practitioner, discuss your blood pressure, especially if your home readings are significantly different than the blood pressure reading at your appointment. Be aware, however, that some variation across blood pressure devices is common.
Watch Your Diet
Two major federally-supported studies concluded that those who eat many fruits and vegetables, whole-grain breads, lower-fat dairy foods and small amounts of meat are the least likely to develop high blood pressure. Following this plan, known as the DASH (Dietary Approaches to Stop Hypertension) diet, has been shown to significantly lower blood pressure. This winning diet is all about balance—in complex carbohydrates, fats, proteins, vitamins and minerals— especially potassium and magnesium.
Get Some Exercise
Exercise is also recommended for reducing hypertension. As little as 30 minutes of walking or other aerobic exercise per day has been shown to reduce blood pressure levels, allowing some people to go off medication. Of course, getting fit also helps you lose weight and relieve stress.
Reduce Stress
Achieving a healthy emotional balance can also reduce blood pressure. Dr. Lark’s patients report success using a variety of non-drug treatments such as meditation, deep breathing and especially biofeedback, a training technique whereby people can learn to improve their health using signals from their own bodies. Dr. Lark describes a British study in which industrial workers with hypertension lowered their blood pressures after only eight weeks using biofeedback.
Seek More Information
We may not know everything there is to know about what causes high blood pressure, but we do know that normal blood pressure can be restored and vascular health improved. Consult with your healthcare practitioner to explore the potential underlying causes and learn about the treatment options available. Be an informed healthcare consumer, and realize that restoring testosterone, progesterone, estrogens, and maintaining thyroid and DHEA may be an important element in creating a healthy vascular system.
The information on this website is for informational purposes only and is not intended to be a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified healthcare provider with any questions you may have regarding any condition or medication. Do not disregard professional medical advice or delay in seeking it because of something you have read on this site.
